


Healthcare organizations across the United States are navigating provider shortages, expanding into new markets, and onboarding clinicians at a pace that their credentialing infrastructure was never designed to support. In that environment, provider credentialing — the formal process of verifying that a clinician is qualified, licensed, and authorized to practice — has become one of the highest-leverage administrative functions in the entire revenue cycle.
Get it right, and providers are billing within weeks of their start date. Get it wrong, and the organization absorbs thousands of dollars in lost revenue per day, per provider, while delayed enrollments quietly accumulate in the background.
This guide covers everything U.S. healthcare executives, compliance officers, and revenue managers need to understand about the provider credentialing process in 2026 — from foundational definitions to the technology changes reshaping how the best organizations manage it.
What Is Provider Credentialing?
Provider credentialing is the structured process by which healthcare organizations, hospitals, and insurance payers verify that a clinician possesses the education, training, licensure, and professional history required to deliver patient care and bill for services rendered.
At its most fundamental level, credentialing answers a single question: Is this provider genuinely qualified to do what they claim they can do?
The answer has consequences that extend in three directions simultaneously. For patients, credentialing is a patient safety mechanism — it ensures that the person treating them holds legitimate, verified qualifications. For healthcare organizations, it is a compliance requirement tied directly to CMS Conditions of Participation and accreditation standards. And for payers, it determines whether a provider is eligible for network participation and reimbursement.
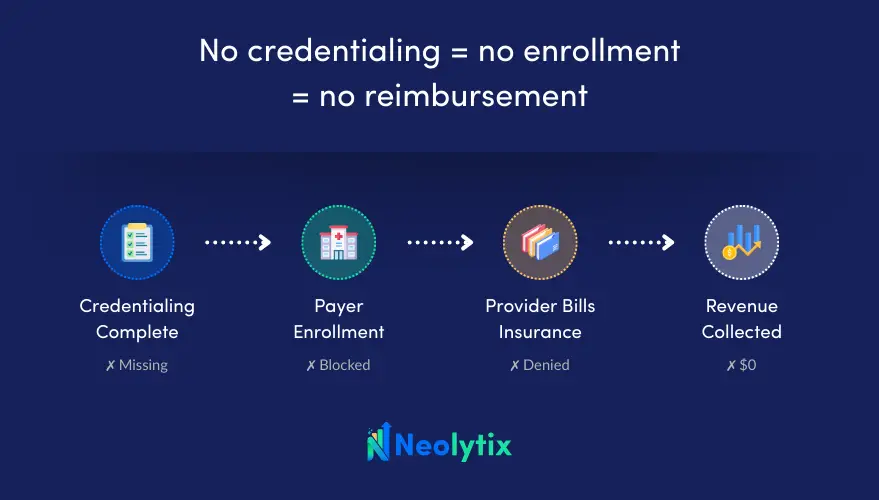
The financial logic is blunt: without completed credentialing, a provider cannot be enrolled with payers. Without enrollment, they cannot bill insurance. And without billing, the organization absorbs the full cost of that provider’s time without collecting revenue. No credentialing = no enrollment = no reimbursement.
It is also important to distinguish credentialing from two related processes that are frequently confused with it. Privileging defines what specific clinical procedures a credentialed provider is authorized to perform at a particular facility — two physicians with identical credentials can receive different privileges based on demonstrated competency and facility-specific resources. Payer enrollment is the downstream contractual process of joining an insurer’s network, which follows credentialing but involves its own separate application, timeline, and approval workflow. For a full breakdown of where credentialing ends and privileging begins, see Credentialing vs. Privileging in Healthcare: Definitions, Differences, and Why Both Matter.
Who Needs Provider Credentialing?
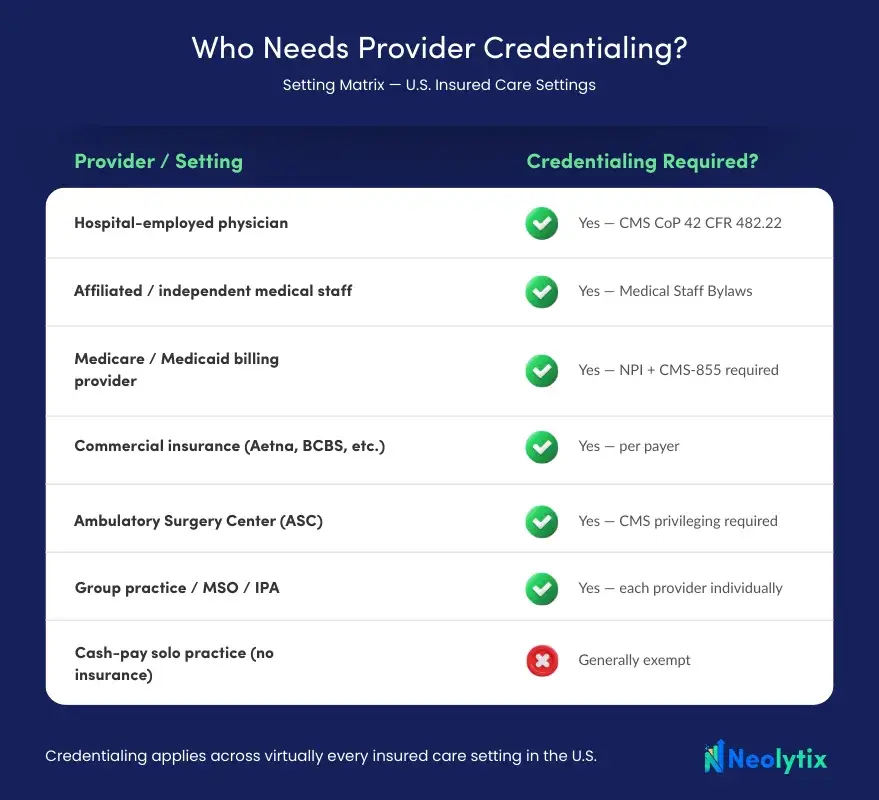
The short answer: any licensed healthcare provider who bills insurance — whether independently or through a facility — will encounter credentialing requirements. The specific form those requirements take depends on the setting.
- Hospitals and health systems are required under CMS Conditions of Participation (42 CFR 482.22) to examine the credentials of all eligible medical staff candidates. This applies to both employed and affiliated providers. It is a Condition of Participation, not optional guidance — non-compliance puts the organization’s entire Medicare and Medicaid reimbursement at risk.
- Medicare and Medicaid require providers to hold an active NPI and complete enrollment applications with supporting credential documentation. The process differs between programs and by state for Medicaid.
- Commercial insurance payers — including United Healthcare, Aetna, Blue Cross Blue Shield, Cigna, and Humana — each conduct their own credentialing review before granting network participation. A provider must be separately credentialed and enrolled with each payer they intend to bill.
- Ambulatory Surgery Centers (ASCs) have their own credentialing and privileging requirements under CMS, particularly for providers performing procedures in those settings.
- Group practices, IPAs, and MSOs must credential each individual provider, even in large multi-provider organizations. There are no shortcuts for volume.
Solo physicians in purely cash-pay private practices who do not accept insurance are generally exempt from institutional credentialing. But for virtually every other clinical setting in the U.S., credentialing is a non-negotiable entry point.
Credentialing is not a one-time event. Re-credentialing is required at minimum every two years to maintain compliance with The Joint Commission, CMS standards, and most commercial payers. Letting credentials lapse — particularly licenses, board certifications, or malpractice coverage — can halt billing and trigger compliance exposure with minimal warning.’
How Does the Provider Credentialing Process Work?
The provider credentialing process follows a consistent framework across settings, though the timeline and complexity vary by organization type, specialty, and payer mix. Here is how it works in practice.
1. Application and Document Collection
The process begins with gathering a complete documentation package from the provider. A standard physician credentialing checklist includes medical school diploma and transcripts; residency, fellowship, and training completion certificates; current state medical licenses for all states where the provider practices; DEA registration (where applicable); board certifications; current malpractice insurance certificate with claims history; a National Practitioner Data Bank (NPDB) self-query; work history covering typically five to ten years; professional references; explanation of any employment gaps; and government-issued identification.
Completeness at this stage is the single largest driver of downstream speed. Incomplete or inaccurate applications — missing dates, name discrepancies, unsigned forms — are the leading cause of processing delays, and many of those delays are entirely preventable.
2. CAQH ProView Registration
CAQH ProView is a free, online, provider-managed database that stores and shares credentialing information with insurance payers — think of it as a single digital credential file that eliminates the need to submit the same documents repeatedly to every insurer. Administered by the Council for Affordable Quality Healthcare, it functions as the centralized credential repository for most commercial payer enrollments in the U.S. Rather than filing separate applications with each payer, providers maintain a single CAQH profile that participating insurers access directly. CAQH profiles must be re-attested — confirmed as current and accurate — every 120 days. Profiles that lapse are one of the most common and most avoidable causes of enrollment failure.
3. Primary Source Verification (PSV)
Primary source verification is the technical and regulatory core of credentialing. It requires independently confirming every credential directly with the original issuing institution — not relying on copies provided by the provider.
Both NCQA (National Committee for Quality Assurance) standards and CMS (Centers for Medicare & Medicaid Services) Conditions of Participation require PSV to be conducted by the credentialing organization or a designated CVO (Credentialing Verification Organization). The following checks take place during this stage:
- Medical education and training — Verified directly with the provider’s medical school, residency program, and fellowship institution
- State medical licensure — Confirmed active and in good standing with the relevant state medical licensing board
- DEA (Drug Enforcement Administration) registration — Verified for providers authorized to prescribe controlled substances
- Board certifications — Confirmed with the issuing specialty board, such as ABIM (American Board of Internal Medicine), ABFM (American Board of Family Medicine), or ABS (American Board of Surgery)
- NPDB (National Practitioner Data Bank) report — Checked for any malpractice payments, adverse clinical privilege actions, or disciplinary sanctions
- OIG (Office of Inspector General) exclusion check — Confirms the provider is not excluded from participating in federal healthcare programs
- SAM (System for Award Management) check — Verifies the provider is not debarred from federal contracts or programs
- Employment and work history — Confirmed with previous employers and professional references
Any discrepancy found during PSV — a name variation, an unaccounted employment gap, an unreported sanction — must be formally resolved before the file advances.
4. Data Review and Gap Assessment
Credentialing specialists conduct a structured review of the verified file, looking for red flags that could delay or disqualify a credentialing application. Common red flags include:
- Malpractice claims — Paid claims or pending suits reported to the NPDB
- Disciplinary actions — License restrictions, probation, or suspension by a state board or hospital
- State board sanctions — Reprimands, consent orders, or conditions placed on a license
- Federal exclusions — Provider listed on the OIG exclusion database or SAM debarment registry
- Employment gaps — Unexplained gaps in work history that require written clarification from the provider
- Inconsistent documentation — Name variations, date discrepancies, or missing records across submitted documents
This is where experienced judgment matters most — identifying what needs follow-up versus what represents a material risk requires expertise that purely administrative processing cannot replicate.
5. Committee Review and Privilege Determination
Once the file is clean and complete, it proceeds to the organization’s medical staff leadership or credentialing committee for review. Committee meetings occur on defined schedules — typically monthly — which means an application that misses a cycle by days can wait 30 additional days regardless of how complete and accurate it is. The committee makes recommendations to the governing body, which formally grants privileges. The provider receives written notification of their credentialing status.
6. Payer Enrollment
Credentialing and enrollment are complementary but distinct. Once primary source verification is complete, enrollment applications must be submitted individually to each payer — Medicare, Medicaid, and commercial insurers each have their own application, portal, and processing timeline. The key is to initiate enrollment as soon as PSV is complete rather than waiting for the full credentialing decision, as running both processes in parallel can reduce total time-to-billing by 45 to 60 days.
For a detailed walkthrough of navigating payer networks and building an enrollment strategy, see How to Get Credentialed with Insurance Companies: Key Strategies.

What Are the Requirements for Provider Credentialing?
Requirements vary by setting, specialty, and state, but the following elements are consistently required across virtually all credentialing bodies in the U.S.:
Credential Element | Verified With |
Medical education and training | Medical school, residency and fellowship programs |
Active state licensure | State medical licensing board |
DEA registration | DEA verification system (where applicable) |
Board certification | Issuing specialty board (ABIM, ABFM, ABS, etc.) |
Malpractice insurance | Issuing insurer; claims history reviewed |
NPDB report | National Practitioner Data Bank |
OIG/SAM exclusion status | Federal exclusion registries |
Employment and work history | Previous employers and professional references |
Criminal background | State/federal databases (requirements vary by payer) |
For federal Medicare and Medicaid participation, providers must also hold a valid NPI (National Provider Identifier) and complete the applicable CMS enrollment form — the CMS-855 series for most provider types. These applications are submitted through the Provider Enrollment, Chain, and Ownership System (PECOS).
State Medicaid programs add another layer, with requirements that vary significantly across states. Providers practicing in multiple states must maintain active licensure and complete enrollment separately in each jurisdiction.
Why Is Provider Credentialing Essential?
Healthcare executives sometimes treat credentialing as a compliance checkbox — something to get through rather than something to get right. That framing understates what is actually at stake.
Patient safety is the foundational reason credentialing exists. A provider with a lapsed license, undisclosed malpractice history, or unverified training is a liability to every patient they treat. Credentialing is the system that prevents that from happening at scale.
Regulatory compliance is non-negotiable. Hospitals that fail to properly credential medical staff risk losing their CMS certification — which means losing Medicare and Medicaid reimbursement entirely. The Joint Commission accreditation, NCQA standards for managed care organizations, and state health department regulations all contain credentialing requirements with real enforcement mechanisms.
Revenue cycle integrity is the dimension most directly visible to CFOs and revenue managers. A provider who is credentialed but not enrolled cannot bill in-network. A provider enrolled with incorrect NPI or taxonomy codes will generate claim denials that may not surface until weeks or months after service delivery — creating retroactive revenue exposure that is difficult and expensive to recover. Organizations that treat credentialing as a revenue function — tracking it with the same rigor as denial rates, days in AR, and clean claim rates — consistently outperform those that treat it as a standalone administrative task.
Legal and liability exposure is significant and often underappreciated. Negligent credentialing claims — where an organization is held liable for harm caused by a provider whose qualifications were not properly verified — represent a meaningful and growing area of healthcare liability.
How Technology Is Transforming Provider Credentialing
The core legal and regulatory requirements of credentialing have not changed, but the operational infrastructure for executing those requirements is being fundamentally redesigned. Four developments define the credentialing technology landscape in 2026.
Automated Primary Source Verification. Leading credentialing platforms now automate PSV for state licenses, DEA registrations, OIG/SAM exclusion checks, and most board certifications. Verification that previously required days of manual outreach and follow-up can now be completed in hours for the majority of credential elements. This shifts the human effort toward exception handling — the cases that genuinely require judgment — rather than routine verification tasks.
Integrated credentialing and enrollment platforms. Historically, credentialing and payer enrollment were managed in separate systems, creating data duplication, handoff delays, and status blind spots between teams. Purpose-built platforms that unify both workflows in a single database enable the parallel processing that accelerates time-to-revenue and eliminate the rework that occurs when enrollment teams are working from incomplete or outdated credentialing data.
Real-time dashboards and predictive tracking. Executive-level visibility into credentialing pipeline — including application status, expected completion dates, flagged exceptions, and provider start-date risk — has shifted from a manual reporting exercise to an automated dashboard function. Organizations using this kind of visibility can accurately forecast provider onboarding timelines, which directly informs operational planning, hiring decisions, and revenue projections. For insight into how this technology trajectory is evolving, see Exploring the Future of Physician Credentialing.
AI-assisted discrepancy detection. Machine learning tools are increasingly capable of flagging application inconsistencies — date discrepancies, name variations, missing documentation — before human review. This shifts error detection earlier in the process, where corrections are less costly and delays are easier to prevent. The practical result is fewer surprises at the committee review stage and faster average credentialing cycles.
Best Practices for Provider Credentialing in 2026
The organizations achieving the fastest, most accurate credentialing outcomes share a consistent set of operational principles.
Start credentialing the day the offer letter is signed. The earlier the process begins, the lower the probability of a gap between a provider’s start date and their ability to bill. Waiting until onboarding is complete to initiate credentialing is one of the most common and most avoidable sources of delay.
Run credentialing and payer enrollment in parallel. Submitting enrollment applications to payers as soon as primary source verification is complete — rather than waiting for the full credentialing decision — is the highest-impact sequencing change most organizations can make. For a step-by-step framework for structuring this workflow, see Step-by-Step Guide to a Successful Medical Credentialing Process.
Maintain CAQH profiles proactively. Assign ownership of CAQH attestation updates on a defined schedule. Reactive maintenance — updating profiles only when a payer flags a lapsed attestation — is a guaranteed source of preventable delays.
Track all credential expiration dates centrally. Every license, certification, malpractice policy, and DEA registration has an expiration date. Automated expiration alerts — rather than manual calendar tracking — are the reliable way to ensure that a single lapsed credential does not trigger a re-credentialing failure mid-cycle.
Standardize your credentialing workflow. Documented, repeatable processes reduce dependency on institutional knowledge held by individual staff members and create consistency across providers, locations, and payer types. This matters especially for multi-site groups and MSOs where credentialing volume is high and staff turnover is a reality.
Evaluate the in-house vs. outsourced decision honestly. For smaller practices managing a handful of providers, in-house credentialing with strong software support can be sufficient. For organizations with ten or more providers, multi-state operations, or rapid onboarding volume, outsourced credentialing with a specialized partner consistently delivers faster cycle times, lower per-provider cost, and stronger payer relationships. The total cost of in-house credentialing — including staff time, software, rework from errors, and delay-related revenue loss — is frequently higher than organizations account for when they make this decision.
For specialty-specific considerations, including the unique requirements for mental health providers, see Medical Credentialing Guide for Therapists and Mental Health Professionals.
Conclusion
Provider credentialing is not a back-office function. It is the operational gateway through which every provider must pass before they can treat patients under an insurance plan, bill for services, or practice within a healthcare organization. Done well, it protects patients, protects the organization from liability, and enables revenue to flow from the moment a provider starts. Done poorly — or slowly — it creates compliance exposure, delays care delivery, and quietly drains revenue that is difficult to recover.
In 2026, healthcare organizations that treat credentialing as a strategic, technology-enabled, revenue cycle-integrated function are moving faster and operating with greater financial predictability than those that treat it as administrative overhead. The foundational process has not changed. The tools, timelines, and competitive stakes have.

Frequently Asked Questions
What is provider credentialing?
Provider credentialing is the formal process by which healthcare organizations, hospitals, and insurance payers verify that a clinician possesses the education, training, licensure, and professional history required to deliver patient care and bill for services. Without completed credentialing, a provider cannot be enrolled with payers — and without enrollment, they cannot bill insurance. It is simultaneously a patient safety mechanism, a regulatory compliance requirement, and a revenue enablement function.
Who needs provider credentialing?
Any licensed healthcare provider who bills insurance must be credentialed. This includes physicians, nurse practitioners, physician assistants, therapists, and other licensed clinicians working in hospitals, health systems, group practices, ambulatory surgery centers, IPAs, and MSOs. Medicare and Medicaid require credentialing and enrollment for all participating providers. Commercial payers — including Aetna, United Healthcare, BCBS, and Cigna — each conduct their own credentialing review before granting network participation. Solo cash-pay physicians who do not accept insurance are generally exempt.
How does the provider credentialing process work?
The provider credentialing process follows six core steps:
- Application and document collection — gathering licenses, certifications, malpractice history, work history, and identification.
- CAQH ProView registration — creating or updating the provider’s centralized credential profile, which participating payers access directly.
- Primary source verification (PSV) — independently confirming every credential with the original issuing institution, such as medical schools, state licensing boards, and certification bodies.
- Data review and gap assessment — reviewing the verified file for red flags such as malpractice claims, employment gaps, or disciplinary actions.
- Committee review and privilege determination — the medical staff committee reviews the completed file and formally grants clinical privileges.
- Payer enrollment — submitting enrollment applications to each insurer, ideally running parallel to credentialing to reduce time-to-revenue
What are the requirements for provider credentialing?
The standard requirements for provider credentialing in the U.S. include:
- Verified medical education and training (medical school, residency, fellowship)
- Active state medical licensure confirmed with the state board
- DEA registration where applicable
- Board certification verified with the issuing specialty board
- Current malpractice insurance with claims history
- A National Practitioner Data Bank (NPDB) report
- OIG and SAM federal exclusion checks
- Employment and work history covering five to ten years
- Criminal background check (requirements vary by payer)
For Medicare and Medicaid enrollment, providers must also hold a valid NPI and complete the applicable CMS-855 enrollment form through PECOS.
Why is provider credentialing essential?
Provider credentialing is essential for three reasons. First, patient safety — it ensures that every clinician treating patients holds verified, legitimate qualifications and has no undisclosed malpractice or disciplinary history. Second, regulatory compliance — CMS Conditions of Participation (42 CFR 482.22) require hospitals participating in Medicare and Medicaid to credential all eligible medical staff; non-compliance risks loss of CMS certification and all associated reimbursement. Third, revenue cycle integrity — a provider who is not properly credentialed and enrolled cannot bill insurance, and errors in credentialing generate claim denials that may not surface until weeks after service delivery, creating retroactive revenue exposure that is costly to recover.
How long does provider credentialing take?
Provider credentialing typically takes between 60 and 120 days from application submission to completed payer enrollment, though timelines vary by organization type, payer, and specialty. Hospital credentialing through a medical staff committee averages 60–90 days when applications are complete. Commercial payer enrollment can add another 30–90 days depending on the insurer’s processing backlog. The most common factors that extend timelines include incomplete applications, lapsed CAQH profiles, slow primary source verification responses, missed committee meeting cycles, and sequential rather than parallel credentialing and enrollment workflows.
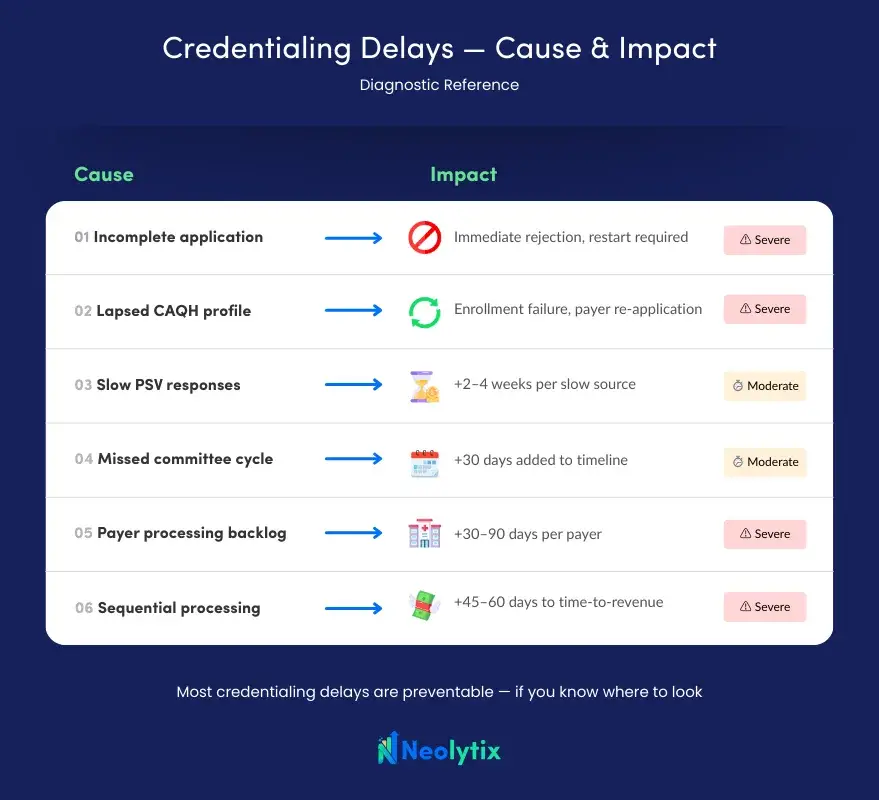
What causes credentialing delays?
The most common causes of provider credentialing delays are:
- Incomplete or inaccurate applications — missing documents, date discrepancies, and unsigned forms are the leading source of processing rejections.
- Lapsed CAQH profiles — providers who miss the 120-day re-attestation window create avoidable enrollment failures.
- Slow primary source responses — some medical schools, international programs, and state boards have long response times that require early outreach.
- Missed committee cycles — medical staff committees meet on fixed monthly schedules; missing a cycle adds up to 30 days regardless of application quality.
- Payer processing backlogs — Medicaid programs and some commercial payers carry multi-month application queues.
- Sequential processing — organizations that wait for full credentialing completion before beginning payer enrollment add 45–60 unnecessary days to time-to-revenue.
How is technology transforming provider credentialing?
Technology is reshaping provider credentialing in four key ways in 2026. Automated primary source verification now completes in hours what previously required days of manual outreach for licenses, DEA registrations, and board certifications. Integrated credentialing and enrollment platforms unify both workflows in a single system, enabling parallel processing that reduces time-to-revenue by 45–60 days. Real-time executive dashboards provide live visibility into application status, expected completion dates, and provider start-date risk — replacing manual spreadsheet reporting. AI-assisted discrepancy detection flags application inconsistencies before human review, shifting error correction to earlier in the process where it is faster and less costly to resolve.



