- Contact Us +1 224 529 4400
- Schedule A Free Consultation
Radiology is the sharp-eyed detective of modern healthcare, sniffing out diagnoses and mapping out treatment plans with pinpoint precision. But when it comes to billing? It’s less Sherlock Holmes and more sudoku with legal consequences.
Coding for radiology isn’t just about knowing CPT, ICD-10-CM, and HCPCS codes, it’s about documenting every detail with surgical accuracy. Miss a step, and you could be looking at claim denials,a compliance headaches, and vanishing revenue.
Why Radiology Coding Matters in 2025
Radiology sits at the heart of healthcare diagnostics, but getting reimbursed for those high-tech scans? That’s where the real challenge kicks in.
With coding guidelines tightening and audits lurking around every corner, accurate radiology coding is more crucial than ever. Think of it as the bridge between life-saving diagnostics and keeping your revenue cycle alive.

Poor documentation is one of the top reasons radiology claims get denied. The fix? Tight, thorough, and coder-friendly notes. Your future self and your bottom line will thank you.

What Is Included in a Radiology Procedure and Coding Evaluation?
Radiology coding is about more than assigning codes, it’s decoding a patient’s medical story through images, reports, and just the right amount of acronyms. Whether it’s a routine chest X-ray or an intricate nuclear scan, each procedure must be backed by solid documentation and coded to perfection.
Precision in Documentation and Coding
Radiology covers a huge range of diagnostic and interventional services, each requiring its own billing finesse. Documenting the right details ensures medical necessity, cleaner claims, and fewer reimbursement hiccups.
Here’s what a strong radiology coding evaluation should include:
Patient History and Clinical Indications
The story starts here: symptoms, past imaging, and relevant health conditions.
This information supports the medical necessity of the radiology procedure and must be clearly reflected in the patient’s record.
Imaging Modality Selection
Radiologists don’t pick tools at random. Each modality comes with its own code (and billing landmines):
Imaging Modality Selection
Used for evaluating fractures, infections, and chest abnormalities.
Computed Tomography (CT)
Picture Provides detailed cross-sectional imaging for trauma, cancer screening, and organ evaluation.
Magnetic Resonance Imaging (MRI)
Used for soft tissue evaluation, neurological conditions, and musculoskeletal injuries.
Ultrasound
Frequently used in obstetrics, vascular studies, and soft tissue imaging.
Nuclear Medicine (PET, SPECT, and Bone Scans)
Assists in functional imaging for oncology, cardiology, and neurology.
Clinical Decision-Making and Report Documentation
Radiologists are storytellers in scrubs. Their reports translate grayscale pixels into life-altering insight. Here’s what needs to be in the report:
- Findings and interpretation of the imaging results.
- Recommendations for further studies if needed.
- Correlation with clinical findings.
- Documentation of contrast use, laterality, and specific anatomical details.
Accurate documentation ensures proper reimbursement and supports medical necessity for any follow-up imaging.
Did you know that radiology coding requires detailed knowledge of both CPT and ICD-10 codes?
Accurate coding is essential for proper reimbursement and compliance with healthcare regulations
Key CPT Codes for Radiology Procedures in 2025
New 2025 Radiology Codes
CPT Code
Description
76014
MR safety implant and/or foreign body assessment by trained clinical staff, including identification and verification of implant components from appropriate sources (eg, surgical reports, imaging reports, medical device databases, device vendors, review of prior imaging), analyzing current MR conditional status of individual components and systems, and consulting published professional guidance with written report; initial 15 minutes
76015
MR safety implant and/or foreign body assessment by trained clinical staff, including identification and verification of implant components from appropriate sources (eg, surgical reports, imaging reports, medical device databases, device vendors, review of prior imaging), analyzing current MR conditional status of individual components and systems, and consulting published professional guidance with written report; each additional 30 minutes (List separately in addition to code for primary procedure)
76016
MR safety determination by a physician or other qualified health care professional responsible for the safety of the MR procedure, including review of implant MR conditions for indicated MR examination, analysis of risk vs clinical benefit of performing MR examination, and determination of MR equipment, accessory equipment, and expertise required to perform examination, with written report
76017
MR safety medical physics examination customization, planning and performance monitoring by medical physicist or MR safety expert, with review and analysis by physician or other qualified health care professional to prioritize and select views and imaging sequences, to tailor MR acquisition specific to restrictive requirements or artifacts associated with MR conditional implants or to mitigate risk of non-conditional implants or foreign bodies, with written report
76018
MR safety implant electronics preparation under supervision of physician or other qualified health care professional, including MR-specific programming of pulse generator and/or transmitter to verify device integrity, protection of device internal circuitry from MR electromagnetic fields, and protection of patient from risks of unintended stimulation or heating while in the MR room, with written report
76019
MR safety implant positioning and/or immobilization under supervision of physician or other qualified health care professional, including application of physical protections to secure implanted medical device from MR-induced translational or vibrational forces, magnetically induced functional changes, and/or prevention of radiofrequency burns from inadvertent tissue contact while in the MR room, with written report
MRI – Monitored Transurethral Ultrasound Ablation (TULSA)
Three new codes were created for the TULSA procedure which delivers predictable physician-prescribed ablation of prostate tissue for treatment of prostate cancer.
Monitored Transurethral Ultrasound Ablation (TULSA)
CPT Code
Description
51721
Insertion of transurethral ablation transducer for delivery of thermal ultrasound for prostate tissue ablation, including suprapubic tube placement during the same session and placement of an endorectal cooling device, when performed
55881
Ablation of prostate tissue, transurethral, using thermal ultrasound, including magnetic resonance imaging guidance for, and monitoring of, tissue ablation
55882
Ablation of prostate tissue, transurethral, using thermal ultrasound, including magnetic resonance imaging guidance for, and monitoring of, tissue ablation; with insertion of transurethral ultrasound transducer for delivery of thermal ultrasound, including suprapubic tube placement and placement of an endorectal cooling device, when performed
Transcranial Doppler study of the Intracranial Arteries
Codes 93896–93898 were created to report procedures performed with a complete transcranial Doppler study of the intracranial arteries
Chest X-Ray procedures
CPT Code
Description
93896
Vasoreactivity study performed with transcranial Doppler study of intracranial arteries, complete (List separately in addition to code for primary procedure)
93897
Emboli detection without intravenous microbubble injection performed with transcranial Doppler study of intracranial arteries, complete (List separately in addition to code for primary procedure)
93898
Venous-arterial shunt detection with intravenous microbubble injection performed with transcranial Doppler study of intracranial arteries, complete (List separately in addition to code for primary procedure)
Percutaneous Radiofrequency Ablation
Chest X-Ray procedures
CPT Code
Description
60660
Ablation of 1 or more thyroid nodule(s), one lobe or the isthmus, percutaneous, including imaging guidance, radiofrequency
60661
Ablation of 1 or more thyroid nodule(s), additional lobe, percutaneous, including imaging guidance, radiofrequency (List separately in addition to code for primary procedure)
Other Common Diagnostic Imaging Codes
Chest X-Ray procedures
CPT Code
Description
71045
Chest X-ray, single view
- A single frontal X-ray used to evaluate the lungs, heart, and ribs.
- Common uses: Infection, chest pain, trauma, or fluid buildup.
71046
Chest X-ray, two views
- Includes posteroanterior (PA) and lateral views for better lung and heart assessment.
- Common uses: COPD, pneumonia, pleural effusion, or post-surgical checks.
71047
Chest X-ray, three views
- Adds an oblique or decubitus view for detailed imaging of small pneumothorax or rib fractures.
- Common uses: Chest trauma, fluid shifts, or pre-surgical evaluation.
Brain and Neck procedures
CPT Code
Description
70551
MRI of the brain, without the use of contrast. This code is used for standard brain imaging to detect abnormalities.
70553
MRI of the brain, with contrast. This enhanced scan provides detailed images to identify issues not visible without contrast.
70540
MRI of the orbit (eye socket), without contrast. Used to examine the eye and surrounding structures for abnormalities.
70543
MRI of the orbit, with contrast. This scan offers a more detailed view of the eye area, highlighting any issues more clearly.
70336
MRI of the temporomandibular joint (TMJ). This code is used for imaging the jaw joint to diagnose TMJ disorders.
Spine Procedures
CPT Code
Description
72141
MRI of the lumbar spine (lower back), without contrast. Utilized for evaluating lower back pain and other lumbar spine conditions.
72156
MRI of the thoracic spine (middle back), without contrast. This code is used for imaging the mid-back region to diagnose spine issues.
72148
MRI of the cervical spine (neck), without contrast. Commonly used to assess neck pain and cervical spine disorders.
72157
MRI of the thoracic spine, with contrast. An enhanced scan for detailed imaging of the mid-back.
72158
MRI of the cervical spine, with contrast. Provides a more detailed view of the neck area for diagnosing more complex conditions.
Joint Procedures
CPT Code
Description
73221
MRI of the lumbar spine (lower back), without contrast. Utilized for evaluating lower back pain and other lumbar spine conditions.
73223
MRI of the thoracic spine (middle back), without contrast. This code is used for imaging the mid-back region to diagnose spine issues.
73721
MRI of the thoracic spine (middle back), without contrast. This code is used for imaging the mid-back region to diagnose spine issues.
73723
MRI of the cervical spine (neck), without contrast. Commonly used to assess neck pain and cervical spine disorders.
73131
MRI of the thoracic spine, with contrast. An enhanced scan for detailed imaging of the mid-back.
73133
MRI of the cervical spine, with contrast. Provides a more detailed view of the neck area for diagnosing more complex conditions.
Extremities procedures
CPT Code
Description
73718
MRI of the thigh, without contrast. This scan is used to evaluate thigh muscles, tendons, and other structures.
73720
MRI of the thigh, with contrast. Provides a more detailed image to identify issues not visible in non-contrast scans.
73218
MRI of the forearm, without contrast. Used to assess injuries and conditions affecting the forearm.
73220
MRI of the forearm, with contrast. Offers enhanced imaging for a clearer diagnosis of forearm issues.
73505
MRI of the foot, without contrast. This scan examines the bones, joints, and soft tissues of the foot.
73507
MRI of the foot, with contrast. Provides detailed images for diagnosing complex foot problems.
Lower Extremity MRI Studies
CPT Code
Description
73718
MRI, lower extremity, without contrast
- Provides high-resolution imaging of bones, joints, and soft tissues.
- Common uses: Ligament tears, meniscus injuries, fractures.
73720
MRI, lower extremity, with contrast
- Enhances visualization of vascular and post-surgical changes.
- Common uses: Tumors, infections, nerve entrapment
Lower Extremity MRI Studies
CPT Code
Description
73718
- Provides high-resolution imaging of bones, joints, and soft tissues.
- Common uses: Ligament tears, meniscus injuries, fractures.
73720
- Enhances visualization of vascular and post-surgical changes.
- Common uses: Tumors, infections, nerve entrapment
Other Common Diagnostic Imaging Codes
Chest X-Ray procedures
CPT Code
Description
71045
Chest X-ray, single view
- A single frontal X-ray used to evaluate the lungs, heart, and ribs.
- Common uses: Infection, chest pain, trauma, or fluid buildup.
71046
Chest X-ray, two views
- Includes posteroanterior (PA) and lateral views for better lung and heart assessment.
- Common uses: COPD, pneumonia, pleural effusion, or post-surgical checks.
71047
Chest X-ray, three views
- Adds an oblique or decubitus view for detailed imaging of small pneumothorax or rib fractures.
- Common uses: Chest trauma, fluid shifts, or pre-surgical evaluation.
Other Common Diagnostic Imaging Codes
Chest X-Ray procedures
CPT Code
Description
71045
Chest X-ray, single view
- A single frontal X-ray used to evaluate the lungs, heart, and ribs.
- Common uses: Infection, chest pain, trauma, or fluid buildup.
71046
Chest X-ray, two views
- Includes posteroanterior (PA) and lateral views for better lung and heart assessment.
- Common uses: COPD, pneumonia, pleural effusion, or post-surgical checks.
71047
Chest X-ray, three views
- Adds an oblique or decubitus view for detailed imaging of small pneumothorax or rib fractures.
- Common uses: Chest trauma, fluid shifts, or pre-surgical evaluation.
Effective pain management requires a precise approach, tailored to the condition, type, and location of pain. From straightforward injections to advanced procedures, accurate coding plays a pivotal role in ensuring proper treatment and reimbursement.
This guide breaks down everything you need to stay current and compliant with pain management coding for 2025.
Why Accurate Pain Management Coding Matters in 2025
For pain management clinics, even a single outdated code can lead to denied claims and lost revenue. The increasing complexity of coding requirements and stricter payer guidelines put practices at financial risk if errors are made. Accurate billing is no longer optional, it’s essential.
| Key Challenges Clinics Face: | |
| Complexity: Navigating evolving CPT and ICD-10 guidelines is time-intensive and error-prone. | Financial Risk: Denials and audits caused by inaccurate billing result in costly repercussions. |
The Solution?
Our 2025 Billing & Coding Guide offers:
- A detailed breakdown of all updates to help you stay compliant.
- Practical tools to streamline your coding process.
- Actionable insights to reduce errors and maximize reimbursements.

Overview of Pain Management Billing Code Categories
To code accurately, it’s crucial to understand the structure of CPT codes and their three primary categories. Each serves a unique purpose in medical billing:
Category I: Codes
These codes have descriptors that correspond to a procedure or service.
Range: 00100–99499.
Example: 20604 – Arthrocentesis with ultrasound guidance for small joints.
Category II: Tracking Codes
Supplemental tracking codes for performance measurement.
Example: 0521F – Documentation of a pain management care plan.
Category III: Temporary Codes
Temporary codes for emerging technologies or procedures.
Example: 0095T – Removal of total disc arthroplasty.
Becoming familiar with them and understanding the category will help with chronic management code selection. It will also assist with coding accuracy and capturing specific codes in addition to the primary code.
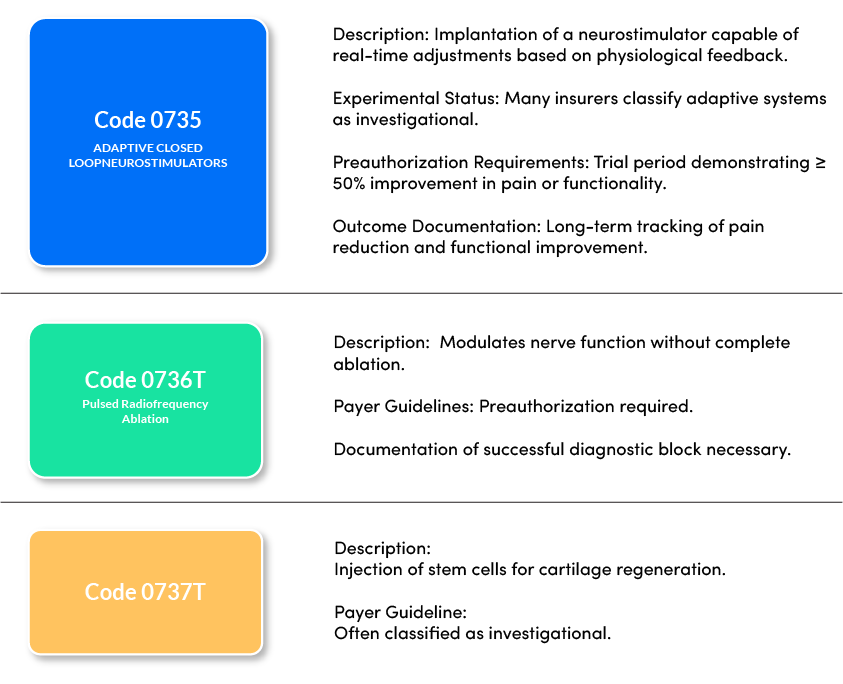
What’s New for 2025?
Here is the outline of the changes done for pain management CPT’s-
- The adoption of minimally invasive techniques like spinal cord stimulators and radiofrequency ablation.
- Integration of imaging guidance into standard procedural codes.
- Expansion into regenerative medicine, reflecting the shift toward biologics and personalized treatments.
Thoracic and Lower Extremity Fascial Plane Block Codes
When it comes to pain management, precision is key. These fascial plane block codes are essential tools for addressing thoracic and lower extremity pain through injections and infusions with imaging guidance.
| Code | Description |
| 64466 | Unilateral thoracic fascial plane block by injection(s), with imaging guidance when performed |
| 64467 | Unilateral thoracic fascial plane block by continuous infusion(s), with imaging guidance when performed |
| 64468 | Bilateral thoracic fascial plane block by injection(s), with imaging guidance when performed |
| 64469 | Bilateral thoracic fascial plane block by infusion(s), with imaging guidance when performed |
| 64473 | Unilateral lower extremity fascial plane block by injection(s), with imaging guidance when performed |
| 64474 | Unilateral lower extremity fascial plane block by infusion(s), with imaging guidance when performed |
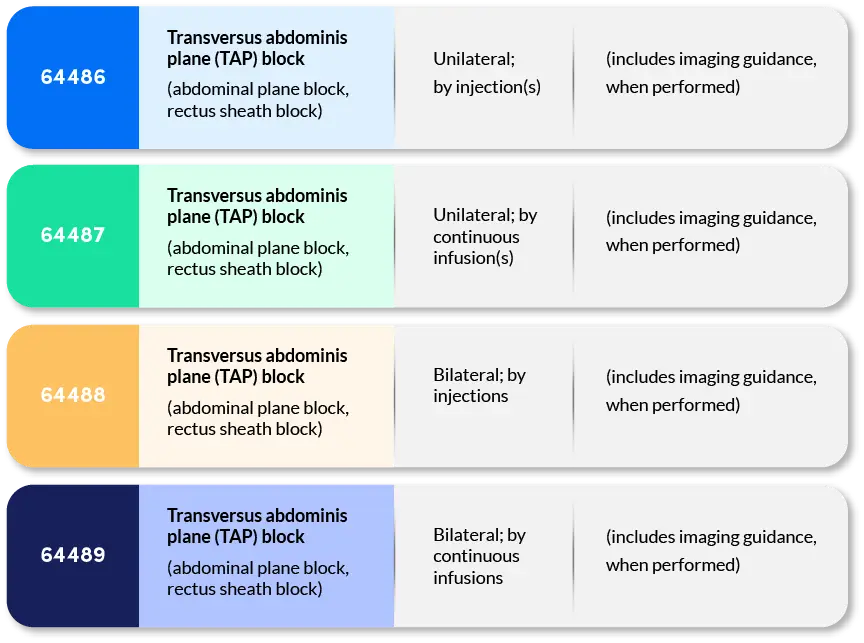
Abdominal Plane Block Codes
Abdominal plane blocks, including TAP and rectus sheath blocks, are critical for managing post-operative and acute abdominal pain. These codes combine injection and infusion procedures with imaging guidance for precise delivery.
Revised Codes
64490 Injection(s), Diagnostic or Therapeutic Agent; Paravertebral Facet Joint or Nerves, Cervical or Thoracic | Revised Descriptor: Imaging guidance is now bundled into the code. Payer Guidelines: Coverage limited to three injections per site annually and Requires documentation of ≥50% temporary pain relief. |
64495 Injection(s), Diagnostic or Therapeutic Agent; Lumbar or Sacral Facet Joint or Nerves | Revised Descriptor: Anatomical descriptions clarified; includes imaging guidance. Payer Guidelines: Diagnostic efficacy must be documented for therapeutic injections. |
64633 Destruction by Neurolytic Agent; Paravertebral Facet Joint Nerve(s), Cervical or Thoracic | Revised Descriptor: Anatomical targets clarified; imaging guidance is now included |
Frequent Pain Management CPT Codes
Accurate CPT coding is the cornerstone of seamless billing and optimized reimbursements. Common treatments often involve injections, nerve blocks, and joint procedures, all requiring precise documentation and coding.
Injections: Relief at the Source Injections are frequently used in pain management to target specific sites such as joints, tendons, or nerves. Trigger point injections are a common treatment for muscle knots caused by tension or injury. Key Codes for Injections:
| Example: For carpal tunnel syndrome (G56.00), a therapeutic injection using CPT 20526 delivers corticosteroids or anesthetics directly to reduce inflammation.
Major Joint Injections:
|
Nerve Blocks: Targeting Pain at Its Source Nerve blocks are a transformative option for managing pain. Providers administer anesthetics or steroids near nerves to numb pain and improve mobility. Key Code for Nerve Blocks: 64405: Greater occipital nerve block for occipital neuralgia (M54.81). | Example: A patient suffering from intense occipital neuralgia receives a targeted injection under CPT 64405 to relieve debilitating headaches caused by nerve trauma. |
ICD-10 Pain Management Codes
Accurate ICD-10 coding ensures compliance and clear communication between providers and payers. Chronic pain conditions are classified using specific codes that reflect the nature and location of the pain.
Key ICD-10 Codes:
- G89.29: Chronic pain, not elsewhere classified.
- M54.5: Chronic low back pain.
- G89.4: Chronic pain syndrome.
Chronic Care Management
Chronic Care Management (CCM) services typically involve non-face-to-face care provided to Medicare beneficiaries with two or more chronic conditions expected to persist for at least 12 months or until the patient’s death. Since CPT guidance can differ from payer reporting requirements, it’s essential to review each payer’s specific policies to ensure compliance.
In the past years we have experienced new changes for CPM (chronic pain management) that took effect January 2023. Some of the changes included an addition of two new HCPCS management codes G3002 and G3003.
CMS recognizes that HCPCS codes G3002 and G3003 are distinct from other care management services like Chronic Care Management. The new chronic pain management and treatment codes are similar to chronic care management codes currently being billed. CPM includes all the services performed each month to help the patient manage their pain.
The code descriptors for each code are listed below:
G3002: Initial 30-minute chronic pain management session, including comprehensive care planning, medication management, and coordination with other specialists.
Specially defined as:
Chronic pain management and treatment, monthly bundle including: diagnosis; assessment and monitoring; administration of a validated pain rating scale or tool; the development, implementation, revision, and/or maintenance of a person-centered care plan that includes strengths, goals, clinical needs, and desired outcomes; overall treatment management; facilitation and coordination of any necessary behavioral health treatment; medication management; pain and health literacy counseling; any necessary chronic pain-related crisis care; and ongoing communication and care coordination between relevant practitioners furnishing care, e.g., physical therapy and occupational therapy, complementary and integrative approaches, and community-based care, as appropriate. Required initial face-to-face visit at least 30 minutes provided by a physician or other qualified health professional; first 30 minutes personally provided by physician or other qualified health care professional, per calendar month. (When using G3002, 30 minutes must be met or exceeded.)
G3003: Each additional 15 minutes of chronic pain management services.
Specially defined as:
Each additional 15 minutes of chronic pain management and treatment by a physician or other qualified healthcare professional, per calendar month (listed separately in addition to code for G3002). When using G3003, 15 minutes must be met or exceeded.
Understanding Pain Management
Mastering essential CPT and ICD-10 codes is key to accurate pain management billing. Codes like G89.29 (chronic pain), M54.5 (low back pain), and G89.4 (chronic pain syndrome) ensure precise documentation, while 99490 covers chronic care management services.
Staying compliant means following up-to-date billing guidelines and leveraging tools like cheat sheets to minimize errors. For chronic back pain, M54.5 is a go-to code, while procedures such as therapeutic injections often use 20526.
Interventional approaches, including 64405 for occipital nerve blocks, are crucial for effective pain management. Similarly, joint and muscle pain treatments commonly rely on 20550 for tendon sheath or ligament injections.
Accurate coding not only ensures compliance but also maximizes reimbursements—keeping your practice efficient and aligned with evolving standards.
Complex Care Management
Complex care management shares common required service elements with CCM but also have different requirements. In addition to the CCM required elements, at least 60 minutes of care must be provided. Another difference is the requirement of moderate to high decision making.
There are common conditions that are typically billed with CCM codes. The chronic conditions include but are not limited to:
- Alzheimer’s disease and related dementia
- Arthritis (osteoarthritis and rheumatoid)
- Asthma
- Atrial fibrillation
- Autism spectrum disorders
- Cancer
- Cardiovascular disease
- Chronic Obstructive Pulmonary Disease (COPD)
- Depression
- Diabetes
- Hypertension
- Infectious diseases like HIV and AIDS
Mastering Complex Care Management
Chronic Care Management (CCM) is essential for effective billing and patient care. Accurately using CPT codes ensures your practice receives proper reimbursement while delivering comprehensive care.
| 99490: Covers at least 20 minutes of clinical staff time directed by a qualified healthcare professional per calendar month. Patients must have two or more chronic conditions expected to last 12+ months or until death, with a significant risk of exacerbation, functional decline, or death. |
| 99491: Reserved for care personally delivered by a physician or other qualified healthcare professional for at least 30 minutes monthly. Includes the same requirements as 99490 but involves direct provider time. |


Pro tip: Pair G2058 with 99490 for an additional 20 minutes of work. Use G0506 for extensive assessments outside the usual scope, billable once per initiating visit
Simplified CCM and Evaluation for Maximum Impact
Complex Care Management takes chronic care a step further, addressing high-complexity cases requiring more provider time and decision-making.
- 99487: Applies to 60-minute care plans that involve moderate-to-high complexity decision-making.
- 99489: Each additional 30 minutes of complex care management directed by a qualified provider.
Documentation Tip: Clear, complete provider notes are critical for accurate code selection and avoiding denials. If records are unclear, query the provider for clarification.

Essential ICD-10 Codes for Pain Management
Understanding and using the correct pain CPT codes is crucial for accurate billing and reimbursement.
Accurate ICD-10 coding is vital for chronic pain documentation. These codes ensure compliance and optimize billing processes. G89.29: Chronic pain, not elsewhere classified. M54.5: Chronic low back pain. G89.4: Chronic pain syndrome. | For nerve blocks, injections, or therapeutic care: 20552: Trigger point injection for 1-2 muscle groups. 64405: Greater occipital nerve block. 20610: Joint aspiration or injection for conditions like osteoarthritis (M19.90). |
Conclusion
Medical coding and billing for chronic pain management can feel overwhelming, with codes spread across different categories and ever-changing guidelines. But you don’t have to tackle it alone.
At Neolytix, we’re here to simplify the process, ensuring your practice stays accurate, compliant, and profitable. Whether you need help with billing, coding, or revenue cycle management, our expert team has you covered. At Neolytix, we provide:
- End-to-end HIPAA-compliant billing solutions.
- Expertise in chronic care and complex care management codes.
- Tailored support to reduce denials and improve revenue.
Let’s make billing easier. Reach out today, and let’s get started on optimizing your practice!