Every time a provider joins a hospital, health system, or multi-site group, two distinct administrative processes must happen before they can see a single patient. Understanding credentialing vs privileging is not just an academic exercise — it is the difference between a compliant, operationally sound onboarding process and one that creates legal exposure, delays, and patient safety gaps.
Yet these two terms are routinely used interchangeably. That confusion has real consequences.
What Is Credentialing in Healthcare?
Credentialing is the process of verifying that a provider is who they say they are — professionally speaking.
It confirms a provider’s education, training, licensure, board certification, work history, and malpractice record. This is done through primary source verification (PSV), which means contacting the original issuing institutions directly — not relying on what the provider self-reports.
Credentialing applies broadly to all clinical staff joining a healthcare organization. It is also the non-negotiable prerequisite for everything that follows — including privileging and payer enrollment.
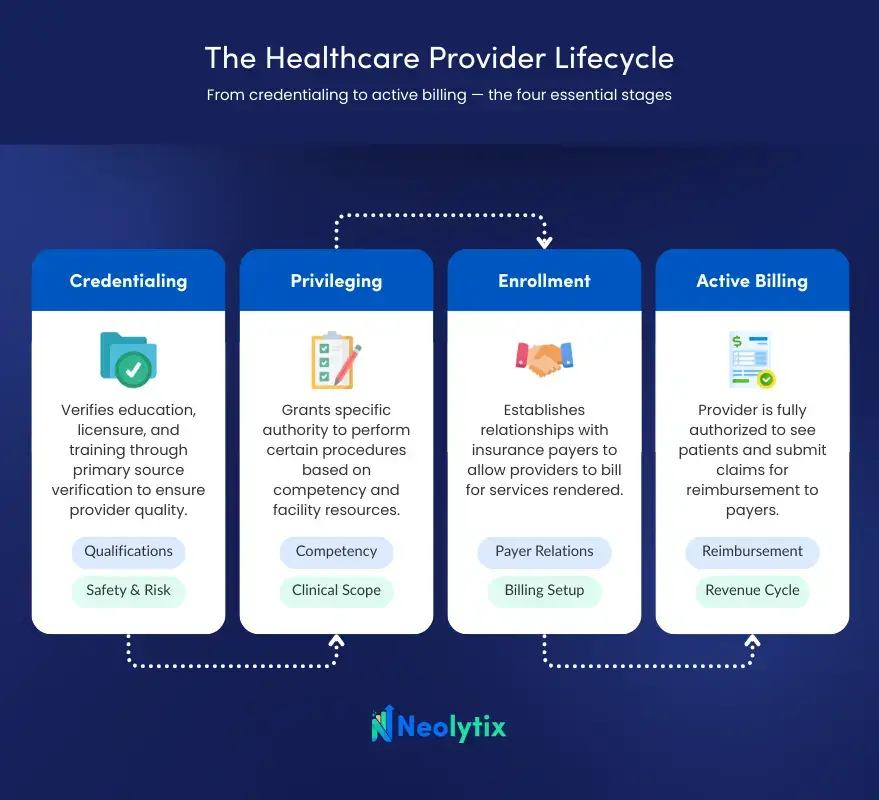
Key Components of the Healthcare Credentialing Process
A complete credentialing file typically includes the following verified elements:
- Education and training — medical school diploma, residency, and fellowship certificates
- Current state licensure — confirmed active and in good standing
- Board certification — verified directly with the issuing board
- DEA registration — where applicable by specialty
- Malpractice history — including any National Practitioner Data Bank (NPDB) flags
- Work history — gaps reviewed and accounted for
- Sanctions and exclusions — OIG exclusion list and federal program checks
Per federal regulations under 42 CFR 482.22, CMS requires hospitals participating in Medicare and Medicaid to examine the credentials of all eligible medical staff candidates. This is a Condition of Participation — not optional.
Re-credentialing is required at least every two years to maintain compliance with both The Joint Commission and CMS standards.
What Is Privileging in Healthcare?
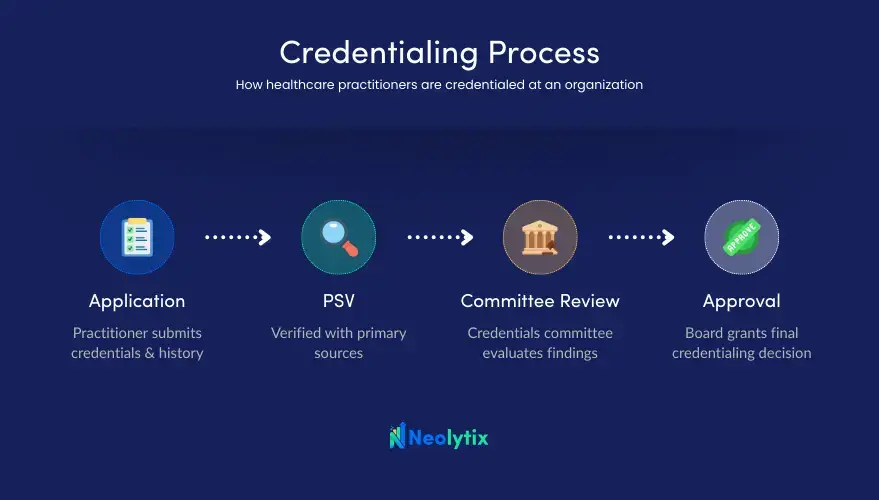
Privileging asks a different, more targeted question: What specific procedures is this provider authorized to perform at this facility?
Where credentialing confirms general qualifications, privileging defines the scope of clinical practice authorized within a specific healthcare organization. Two surgeons can hold identical credentials and still receive different privileges — based on demonstrated competency, case volume, peer review outcomes, and the resources available at that facility.
Privileges are granted by the organization’s medical staff leadership and governing body. They are facility-specific. A provider credentialed at one hospital cannot automatically perform the same procedures at another.
- Neolytix • MC & CVO
Medical Credentialing & CVO
Neolytix manages the complete credentialing lifecycle from primary source verification to payer approvals and revalidation, ensuring your providers are enrolled accurately and activated without unnecessary delays.
Key Aspects of the Healthcare Privileging Process
Privileging decisions are built on more than paperwork. They require an active clinical assessment:
- Scope of practice definition — the exact procedures, treatments, or services a provider is authorized to perform, ranging from broad categories (e.g., general surgery) to highly specific ones (e.g., laparoscopic cholecystectomy)
- Competency assessment — case logs, peer recommendations, and outcomes data reviewed beyond credentials alone
- Facility-specific considerations — available equipment, support staff, and organizational resources factor directly into what privileges are granted
- Governing body approval — medical staff leadership and the executive board authorize all privilege decisions
- Ongoing performance monitoring — through OPPE (Ongoing Professional Practice Evaluation) and FPPE (Focused Professional Practice Evaluation), performance is assessed continuously between renewal cycles
Per CMS guidelines, privileging is specifically required for providers performing medical services within a hospital or ambulatory surgery center (ASC). Common privilege categories include admitting, courtesy, and surgical privileges. Like credentialing, privileges are renewed on a two-year cycle.
Credentialing vs Privileging: The Core Differences at a Glance
| Credentialing | Privileging |
Purpose | Verify general qualifications | Authorize specific clinical procedures |
Scope | All clinical staff | Hospital/ASC-based providers |
Who grants approval | Credentialing committee | Medical staff leadership & governing body |
Basis for decision | Education, licensure, history | Competency, case volume, peer review, facility resources |
Facility-specific? | No | Yes |
Renewal cycle | Every 2 years | Every 2 years |
The clearest way to think about it: credentialing is the key. Privileging is the lock it must fit. Both are required. Neither replaces the other.
Challenges: Why Confusing Credentialing and Privileging Creates Operational Risk
When healthcare administrators treat these as the same process, gaps emerge fast.
A provider may be credentialed — legally verified — but not yet privileged to perform the procedures their role requires. That misalignment stalls care delivery and creates liability before the provider sees their first patient.
The consequences are well-documented. A Wisconsin surgical case cited by Symplr resulted in patient paralysis and subsequent litigation after a hospital failed to properly verify a surgeon’s credentials. The physician had misrepresented board certification and had malpractice restrictions at other facilities — none of which was caught through proper PSV.
Compliance risk compounds the operational problem. NCQA’s updated credentialing standards now require shorter verification timelines, stronger data integrity, and clear audit trails. Inconsistent or poorly documented privileging processes are one of the most common findings during Joint Commission surveys.
For Medical Staff Services Directors managing high provider volumes across multiple sites, this is not a theoretical problem. It is a day-to-day operational reality with measurable downstream impact on patient safety and revenue.
How Credentialing and Privileging Work Together
These two processes are sequential and interdependent — not parallel or interchangeable.
Credentialing always comes first. It establishes the verified foundation on which all subsequent decisions are made. Once a provider’s qualifications are confirmed, privileging uses that information — layered with clinical performance data — to define what that provider can actually do within a specific facility.
Think of it as a two-stage clearance system. The first stage confirms the provider meets baseline standards. The second stage determines precisely where and how they can practice within the organization.
Relias describes this relationship clearly: credentialing confirms a provider is qualified in general, while privileging defines the scope of practice allowed within a specific facility. One cannot function properly without the other.
When both processes are well-coordinated, healthcare organizations onboard providers faster, reduce compliance exposure, and maintain consistent standards of care across locations.
| Credentialing | Privileging |
Core question | Is this provider qualified? | What can this provider do here? |
Process type | Verification | Competency authorization |
Scope | Organization-wide or payer-network | Facility-specific |
Applies to | All providers | Providers performing specific procedures |
Primary inputs | Education, licensure, sanctions, work history | Procedure logs, proctoring, peer references |
Output | Medical staff membership | Delineation of privileges (DOP) |
Governed by | NCQA, CMS, state boards | TJC, CMS Conditions of Participation |
Renewal cycle | Every 2–3 years | Every 2 years (at reappointment) |
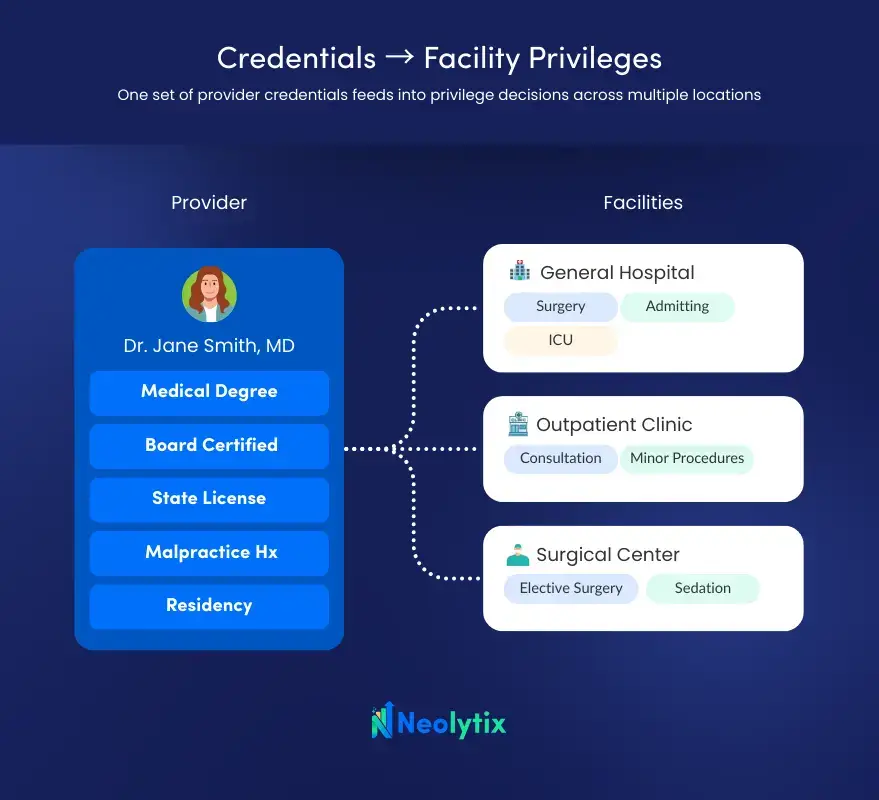
How Credentialing and Privileging Connect to Provider Enrollment
A third process often enters this conversation: provider enrollment. While credentialing and privileging govern clinical authorization within a healthcare organization, enrollment governs a provider’s ability to bill payers — including Medicare, Medicaid, and commercial insurers.
All three are sequential and interdependent. Credentialing provides the verified foundation. Privileging defines the clinical scope. Enrollment unlocks reimbursement. A delay or error in any one of them stalls the others.
Healthcare organizations that manage all three through a coordinated workflow — rather than treating them as separate administrative silos — reduce onboarding delays and eliminate the revenue gaps caused by billing holds during enrollment lag.
How Neolytix Supports Credentialing and Provider Enrollment
Managing credentialing, privileging, and enrollment at scale is complex. It requires precise documentation, clear renewal tracking, multi-source verification, and constant alignment with evolving payer and accreditation requirements.
Neolytix’s NCQA-ready CVO Credentialing Services handle the end-to-end primary source verification process — reducing administrative burden on internal medical staff teams while maintaining audit-ready documentation standards. The process is built for healthcare organizations managing high provider volumes across single or multiple sites.
On the enrollment side, Neolytix’s Provider Enrollment Services ensure providers are actively enrolled with all relevant payers before their first billable date — closing the gap between clinical authorization and revenue activation.
For Medical Staff Services Directors and Compliance Officers managing credentialing and privileging workflows, having a partner who understands both the regulatory and operational dimensions of this process is not a luxury. It is a practical necessity.
- Neolytix • Contact Us
Contact Us
Neolytix partners with healthcare organizations across revenue cycle, credentialing, and administrative operations, 14+ years of expertise and AI-enabled automation to reduce inefficiencies and drive sustainable growth.
Frequently Asked Questions
What is the main difference between credentialing and privileging in healthcare?
Credentialing verifies a provider’s general qualifications — education, licensure, board certification, and history. Privileging determines the specific clinical procedures that provider is authorized to perform at a particular facility. Credentialing applies to all clinical staff; privileging is facility-specific and applies primarily to hospital and ASC-based providers.
Does credentialing always come before privileging?
Yes. Credentialing is always completed first. A provider must be credentialed before any privileging decisions can be made. Privileging decisions are built on the verified information gathered during credentialing.
Are credentialing and privileging required by law?
Federal regulations under 42 CFR 482.22 and 482.12 require hospitals participating in Medicare and Medicaid to credential all medical staff and implement a privileging process. CMS compliance is a Condition of Participation. The Joint Commission also requires both processes for accredited organizations.
How often do credentialing and privileging need to be renewed?
Both are renewed on a two-year cycle. For facilities maintaining Federal Tort Claims Act (FTCA) deeming status, re-credentialing and re-privileging every two years is a federal requirement. Ongoing performance monitoring through OPPE and FPPE continues between renewal cycles.
Can a provider have privileges at one hospital but not another?
Yes. Privileges are facility-specific. A provider must apply for and be separately evaluated for privileges at each individual facility. Credentials do not automatically transfer between institutions.
What is the role of the NPDB in credentialing?
The National Practitioner Data Bank (NPDB) is queried during initial credentialing and re-credentialing. It contains records of malpractice payments, license restrictions, privilege revocations, and federal program exclusions. Hospitals are required to query the NPDB when granting or renewing privileges.
How does provider enrollment differ from credentialing and privileging?
Credentialing verifies clinical qualifications. Privileging authorizes clinical scope within a facility. Enrollment establishes a provider’s relationship with payers — enabling billing for Medicare, Medicaid, and commercial insurance. All three are interdependent, but each serves a distinct administrative and regulatory function.